Hip Arthritis (Osteoarthritis)
Hip arthritis is the leading cause of hip replacement surgery in the UK. If groin pain, morning stiffness, or a failing hip is limiting your daily life, Mr Shakir Hussain (Consultant Orthopaedic Surgeon at the Royal Orthopaedic Hospital Birmingham) offers both total hip replacement and hip resurfacing to patients across Birmingham and the West Midlands, matched to your age, activity level, and anatomy. With over 5,000 procedures performed and a Doctify rating of 4.98/5, he has the experience to get you back to the life you want.

What is hip arthritis?
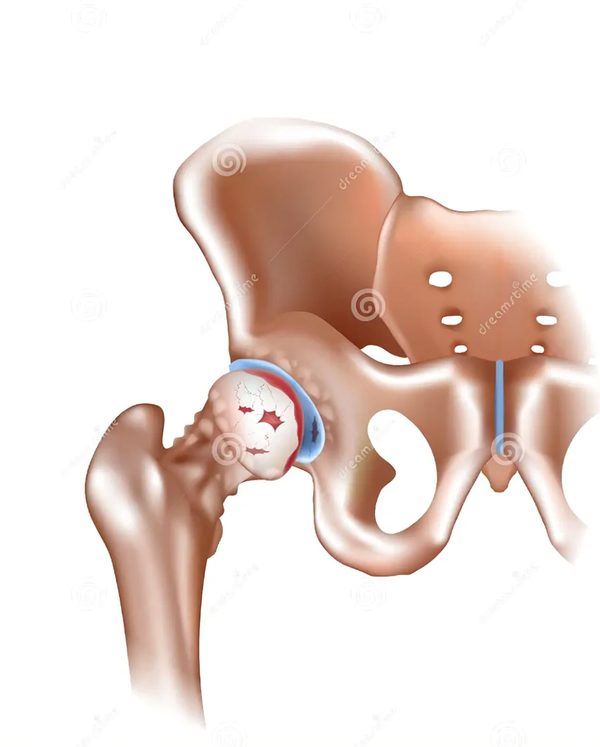
Hip osteoarthritis is the gradual loss of articular cartilage in the hip joint. Without cartilage to cushion the joint, bone rubs on bone, causing groin pain, stiffness, and limp. It is distinct from inflammatory arthritis (such as rheumatoid arthritis), which involves the immune system attacking the joint lining.
The hip is a ball-and-socket joint formed by the femoral head (the top of the thigh bone) and the acetabulum (the socket in the pelvis). In a healthy hip, smooth articular cartilage coats both surfaces, allowing pain-free movement through a wide range of motion.
In hip osteoarthritis, this cartilage thins over years to decades. As it wears away, the joint capsule thickens, the body forms bone spurs called osteophytes, and the underlying bone reacts by becoming denser. The cumulative effect is pain, restricted motion, and progressive disability.
Hip arthritis is the most common reason for hip replacement surgery in the UK. The National Joint Registry recorded over 100,000 primary hip replacements in 2024, the majority for osteoarthritis.
What does hip arthritis pain feel like?
Hip arthritis typically causes a deep, aching pain in the groin or front of the thigh that worsens with walking, stairs, and getting up from a seated position. Morning stiffness lasts less than 30 minutes. Many patients also describe pain referred to the knee, even though the hip is the source.
The pain of hip osteoarthritis follows recognisable patterns that an experienced orthopaedic surgeon will identify quickly. Symptoms tend to build slowly over months or years, sometimes punctuated by flares lasting days to weeks.
Groin pain
Deep, aching pain in the groin and front of the thigh is the classic site. Many patients point to this area when asked where their hip hurts.
The C-sign
Patients often cup the affected hip with thumb on the groin and fingers over the side of the hip, forming a "C" shape, to describe their pain.
Morning stiffness under 30 minutes
Stiffness on first getting out of bed, easing within half an hour as the hip warms up. Stiffness lasting longer suggests inflammatory arthritis instead.
Pain referred to the knee
The hip can refer pain to the knee. Some patients are treated for "knee pain" for months before the true source is recognised.
Reduced walking distance
The distance you can walk before needing to stop steadily shortens. This is a useful marker of progression and of when surgery is appropriate.
Limp and night pain
A visible limp develops as the hip stiffens. Pain that wakes you at night signals advanced disease and is one of the strongest indications for hip replacement.
What causes hip arthritis?
Hip arthritis develops when the cartilage in the hip joint wears down faster than the body can repair it. This can happen with age and use (primary osteoarthritis), or as a consequence of an earlier hip problem such as dysplasia, hip impingement, or a previous fracture (secondary osteoarthritis).
For many years osteoarthritis was assumed to be a simple consequence of ageing. Modern imaging has shown that a large proportion of so-called primary osteoarthritis is actually secondary to subtle structural problems present from childhood or adolescence: mild hip dysplasia, where the socket is shallower than normal, or femoroacetabular impingement, where extra bone on the femoral neck pinches the socket rim and damages cartilage over years of normal activity.
The most important risk factors are:
- Age over 45. Cartilage repair declines with age and lifetime cumulative load adds up.
- Body Mass Index over 29. Each pound of body weight transmits roughly four pounds of force through the hip with every step.
- Previous hip injury. A prior fracture, dislocation, or significant sports injury changes joint mechanics permanently.
- Hip dysplasia. A shallow socket present from birth is responsible for up to 20 to 40 per cent of hip osteoarthritis cases.
- Femoroacetabular impingement (FAI). Cam or pincer deformities cause repetitive cartilage damage with normal activity.
- Family history. Both dysplasia and FAI can be inherited; first-degree relatives of patients with hip osteoarthritis have a measurably higher risk.
- Heavy-loading occupations. Years of farming, manual labour, or other repetitive heavy loading accelerate cartilage wear.
How is hip arthritis diagnosed?
For patients aged 45 and over with activity-related groin pain and morning stiffness under 30 minutes, NICE guidance permits a clinical diagnosis without imaging. An AP weight-bearing pelvic X-ray confirms the diagnosis and grades severity using the Kellgren-Lawrence scale from 1 (doubtful) to 4 (severe).
Diagnosis begins with a careful clinical history and examination. Mr Hussain will ask about the location and quality of your pain, how far you can walk, how your sleep is affected, and what activities you have given up. Examination tests the hip's range of motion, particularly internal rotation, which is usually the first movement to be lost in osteoarthritis. The FABER test and the Stinchfield resisted straight-leg raise help distinguish hip-origin from spine-origin pain.
Imaging confirms the diagnosis and grades severity:
- AP weight-bearing pelvis X-ray. The gold-standard imaging. It shows joint space narrowing, subchondral sclerosis (bone-thickening under the cartilage), subchondral cysts, and osteophytes (bone spurs).
- Kellgren-Lawrence grading. Grade 1 doubtful, Grade 2 mild (definite joint-space narrowing and osteophytes), Grade 3 moderate (marked narrowing, sclerosis, cysts), Grade 4 severe (gross loss of joint space, large osteophytes, deformity).
- MRI. Reserved for atypical presentations, suspected avascular necrosis, or assessment of labral tears in younger patients.
- CT scan. Used for surgical planning in complex cases or where revision surgery is anticipated.
- Blood tests. Only ordered if there is reason to suspect an inflammatory or septic cause: stiffness over 30 minutes, systemic symptoms, or atypical features.

Can hip arthritis be treated without surgery?
No, cartilage damage cannot be reversed. However, structured exercise, weight loss, and topical anti-inflammatory medication can control symptoms for months to years in mild to moderate disease. NICE 2026 guidance has downgraded routine use of paracetamol and does not recommend opioids for osteoarthritis pain.
Non-surgical treatment is appropriate for most patients with mild to moderate hip arthritis. NICE published an updated osteoarthritis guideline (NG226) which made several significant changes to first-line care:
- Therapeutic exercise. Tailored physiotherapy combining strengthening, range-of-motion work, and aerobic exercise. The strongest evidence base of any intervention.
- Weight loss. Every pound of body weight lost reduces force through the hip by roughly four pounds per step. A reduction of at least 5 per cent of body weight is the minimum target.
- Topical NSAIDs. Preferred over oral NSAIDs because of fewer systemic side effects.
- Oral NSAIDs. Used at the lowest effective dose for the shortest duration, with attention to kidney function and stomach lining.
- Paracetamol. NICE 2026 no longer routinely recommends paracetamol for osteoarthritis pain (a notable change from earlier guidance), citing lack of effectiveness.
- Opioids. Not routinely recommended for osteoarthritis pain.
- Intra-articular injections. Image-guided corticosteroid gives short-term pain relief, typically up to three months. Hyaluronic acid offers modest four-to-six month benefit in selected patients. Platelet-rich plasma and combination injections continue to be studied.
Non-surgical treatment becomes futile when the hip has reached Kellgren-Lawrence grade 3 or 4, when night pain disrupts sleep, when walking distance falls below 100 metres, or when three to six months of structured care has failed to control symptoms. At that point, hip replacement becomes the right next step.
If you take prescribed medication, particularly blood-thinners, anti-inflammatories, or rheumatology drugs, please review Mr Hussain's patient guide on medications to pause before hip or knee surgery as you approach a surgical decision.
When should I consider hip replacement?
Hip replacement becomes the right choice when conservative treatment has been tried for three to six months and pain still substantially affects daily life, walking distance is reduced below 100 metres, sleep is disturbed by night pain, or imaging shows end-stage (Kellgren-Lawrence grade 3 to 4) disease.
There is no single test that says it is time for surgery. The decision is made jointly between you and your surgeon, based on how much your hip is affecting your life. The NICE NG226 guideline summarises the threshold as referral for joint replacement when "symptoms have a substantial impact on quality of life and non-surgical management is ineffective or unsuitable".
Practical markers Mr Hussain looks for in consultation:
- Pain that wakes you at night, more than twice a week
- Walking distance reduced to under 100 metres before needing to stop
- Inability to put on your own socks and shoes
- Pain on standing up from a chair or getting out of a car
- Three to six months of structured physiotherapy and medication that has not controlled symptoms
- Imaging showing Kellgren-Lawrence Grade 3 or 4 disease
- Withdrawal from activities you previously enjoyed
Earlier surgery may be appropriate in young, active patients where waiting risks deconditioning, loss of bone stock, or worsening compensatory changes in the spine and knees.
Private consultations with Mr Hussain are available at the Royal Orthopaedic Hospital, Priory Hospital Edgbaston, and Harborne Hospital. See the private consultation and surgery fees page for self-pay pricing and the list of recognised insurers, or book a consultation directly.
Hip replacement or hip resurfacing: which is right for me?
Mr Hussain offers both total hip replacement and hip resurfacing. Total hip replacement suits most patients, particularly those over 60, women, or with reduced bone quality. Hip resurfacing is the bone-preserving option best suited to active men under 60 with good bone quality and a femoral head measuring 48 millimetres or larger.
Both operations relieve the pain of hip arthritis and restore movement, but they differ in how much bone is removed and which patient group does best. Mr Hussain trained in both techniques and offers each based on what is right for the individual patient.
Total Hip Replacement
The femoral head and the acetabulum are both replaced with prosthetic components. A metal or ceramic ball on a stem replaces the head, and a cup with a polyethylene or ceramic liner replaces the socket.
- Suitable for nearly all patients with hip arthritis
- Modern implants designed for 25 to 30 year lifespan
- Day-case surgery available for suitable patients
- Cemented or uncemented fixation tailored to bone quality
- Preferred for patients over 60, women, or with osteoporosis
Hip Resurfacing
Only the surface of the femoral head is capped; the socket is lined. The femoral neck and most of the head are preserved, which keeps options open for the future and offers a more stable joint for high-impact activity.
- Best for active men under 60 with good bone quality
- Requires a femoral head measuring 48 millimetres or larger
- 15-year survivorship of 95.8 per cent in this group (2025 data)
- Lower dislocation risk than total replacement
- Easier conversion to a standard replacement if ever needed
For a more detailed patient comparison covering recovery, return to sport, and implant choice, read Mr Hussain's patient guide on hip resurfacing versus total hip replacement. Active patients may also find returning to sport after hip resurfacing useful for setting realistic expectations.
How successful is hip replacement for arthritis?
Modern hip replacement is one of the most successful operations in medicine. Patient satisfaction is between 80 and 93 per cent. A 2026 Lancet meta-analysis of around two million procedures found 94 per cent of hip replacements were still functioning at 20 years, 93 per cent at 25 years, and 92 per cent at 30 years.
Hip replacement has transformed the lives of millions of patients with arthritis. The combination of refined surgical technique, better implant materials, faster anaesthetic protocols, and same-day mobilisation has produced steady year-on-year improvements in both function and longevity. The National Joint Registry's 22nd Annual Report (2025) confirmed continued year-on-year reduction in revision surgery rates across England, Wales, Northern Ireland, and the Isle of Man.

Expertise in hip arthritis treatment in Birmingham
Consultant at the Royal Orthopaedic Hospital
Mr Hussain practises at the Royal Orthopaedic Hospital Birmingham, one of the largest specialist orthopaedic hospitals in Europe, alongside Priory Hospital Edgbaston and Harborne Hospital.
3,000+ joint replacement cases
From a total of more than 5,000 procedures performed, giving the operative volume and case complexity required for consistently excellent outcomes. Read more about Mr Hussain's training and background.
British Hip Society Travelling Fellowship
Trained at ENDO-Klinik Hamburg under Professor Thorsten Gehrke and Professor Mustafa Citak, the international reference centre for complex hip surgery.
Both hip replacement and hip resurfacing
Many surgeons offer only one technique. Mr Hussain trained in both, allowing the choice to be tailored to the individual patient rather than to a single technique.
Doctify Outstanding Patient Experience 2024, 2025, and 2026
Awarded in three consecutive years, recognising consistently high patient-reported outcomes and communication.
4.98 out of 5 from verified reviews on Doctify. Outstanding Patient Experience Award 2024, 2025, and 2026.
Frequently asked questions about hip arthritis
For more questions about surgery, recovery, fees, and what to expect, see the full frequently asked questions page or read recent patient testimonials.