The Patient
A man in his late fifties presented to Mr Hussain's clinic at the Royal Orthopaedic Hospital in Birmingham with severe, debilitating right hip pain. He had been struggling for some time, and X-rays confirmed end-stage osteoarthritis. The cartilage in his right hip had worn away completely, leaving bone grinding on bone.
What made this case particularly complex was his medical history. He had already undergone significant spinal surgery: a multi-level lumbar spinal fusion extending from L3 all the way down to the sacrum (S1), with interbody fusions at two levels. A complication, fracture of both S1 screws, had added further complexity. He was also an insulin-dependent diabetic with high blood pressure, kidney impairment, and a BMI placing him in the obese range.
To add another dimension: he had already had his left hip resurfaced four years earlier by a different surgeon, and that hip was performing extremely well. Metal ion levels, a key safety marker for hip resurfacing, were well within safe limits.
"The question was not simply whether to operate. The question was which operation gave this patient the best chance of a good, durable outcome, given everything his spine had already changed about his anatomy."
Mr Shakir Hussain, Consultant Orthopaedic SurgeonWhy Spinal Fusion Makes Hip Surgery More Complicated
To understand the challenge, it helps to think of the lower spine, pelvis, and hips not as separate structures, but as a single, interconnected system. Orthopaedic surgeons call this the spinopelvic complex, and it behaves in a remarkably co-ordinated way during everyday movement.
When you sit down from a standing position, several things happen simultaneously. Your hip bends, your lower spine flexes slightly, and (critically) your pelvis tilts backwards. This backward tilt of the pelvis is not incidental; it automatically increases the angle at which the hip socket faces, creating more clearance for the ball of the hip joint and reducing the risk of the two sides jamming together or dislocating.
Think of it like a door hinge that adjusts its own angle depending on how wide you need the door to open. The pelvis is the hinge, and it is supposed to be dynamic.
Spinal fusion permanently stiffens the lumbar spine and reduces the pelvis's ability to tilt backwards when sitting. The result: the hip socket is effectively locked in a fixed position, unable to adapt to the demands of daily movement. For a patient about to receive a new hip joint, this creates a significantly elevated risk of dislocation: the ball slipping out of the socket.
The research evidence is stark. Studies have consistently shown that patients who have a hip replacement after spinal fusion are at substantially higher risk of complications than those without spinal surgery. The dislocation risk in particular can be several times higher, and long fusion constructs (like our patient's L3-to-S1 fusion) carry the greatest risk of all, because they lock the pelvis more rigidly than shorter fusions do.
What the Pre-Operative X-Ray Showed
The pre-operative pelvis X-ray shows bilateral end-stage osteoarthritis. Both hip joint spaces have completely disappeared (the hallmark of severe wear), with bone spurs (osteophytes) visible around the sockets and on the necks of the femurs. Centrally, the spinal fusion metalwork is visible: rods and screws traversing the lumbar spine and anchoring into the sacrum. This hardware is what stiffens the lower spine and pelvis, and it is what makes hip surgery in this patient significantly more demanding than a routine case.

Both hips show end-stage osteoarthritis, with complete loss of joint space, subchondral bone changes and osteophyte formation around the femoral heads and acetabular rims. Centre: lumbar spinal fusion metalwork, L3 to S1, with interbody cages at two levels.
Why Resurfacing, Not Standard Replacement, Was the Right Choice
Here is the counterintuitive insight at the heart of this case. In most clinical discussions, a complex background like this patient's (multiple comorbidities, previous spinal surgery, elevated surgical risk) would suggest choosing the more conservative, more familiar option: a standard total hip replacement.
But for this patient, the standard option was actually the riskier one.
The reason comes back to the dislocation problem. A standard total hip replacement uses a ball that is considerably smaller than the natural femoral head. This is fine in most patients, because the pelvis can compensate by adjusting its angle during movement, keeping the smaller ball safely seated in the socket. But in a patient whose pelvis cannot adjust, because the spine above it is fused solid, a smaller ball means a meaningfully higher chance of dislocation. In this patient, with a long L3-to-S1 fusion, that risk would have been substantially elevated.
Smaller ball → higher dislocation risk
In spinal fusion patients, the pelvis cannot tilt to protect a smaller femoral head. Dislocation risk is 2–4× higher than in patients without fusion, and potentially higher still with long lumbosacral constructs.
Full-size ball → inherently more stable
Resurfacing caps the natural femoral head rather than replacing it, retaining the full natural ball size. This dramatically reduces dislocation risk, a critical advantage when the pelvis cannot compensate dynamically.
Hip resurfacing takes a fundamentally different approach. Rather than removing the femoral head entirely, the surgeon shapes it and caps it with a metal covering, preserving the natural size of the ball. Because the ball is larger (closer to the patient's own anatomy), it is much harder to dislocate, regardless of what the pelvis is doing. Studies show that dislocation rates after hip resurfacing are approximately ten times lower than after standard hip replacement.
For a patient with a stiff, fused spine and a pelvis that cannot adapt, this distinction is clinically decisive.
There was a further advantage specific to this patient's situation. He already had a successful resurfacing on the left side. Matching procedures on both hips means symmetrical biomechanics: the same type of bearing surface, the same ball size, the same functional feel. Had a standard replacement been placed on the right, the two hips would have been dissimilar in ways that can cause subtle imbalances in gait and loading over time.
Finally, there is the long-term consideration. Hip resurfacing preserves the bone of the femoral head. Should revision surgery ever be needed in future (which, in a man in his late fifties with many active decades ahead, is a real possibility), there is substantially more bone available to work with than if a standard replacement had been performed. This is not a trivial point: revision surgery after a failed resurfacing is considerably more straightforward than revision after a failed standard replacement where bone has already been sacrificed.
The Surgical Planning Challenge
Choosing hip resurfacing was the right decision, but it made the technical demands of the surgery considerably higher, not lower.
Hip resurfacing is a more exacting procedure than standard hip replacement even in straightforward cases. The margin for error in the positioning of the socket (acetabular cup) is narrower. If the cup angle is not precisely right, metal ions can be released at elevated rates: a risk specific to the metal-on-metal bearing surface used in resurfacing. In a patient whose fixed pelvis changes the reference geometry that surgeons normally rely on, templating and planning must account for those altered relationships from the outset.
Mr Hussain's pre-operative planning included careful X-ray templating, assessment of the spinal fusion construct and its effect on pelvic positioning, and confirmation of the femoral head morphology to ensure it was suitable for resurfacing. The operation note records that the femoral head shape was satisfactory, that the guidewire was checked in both planes to ensure optimum position, and that a double-check was performed to avoid notching the femoral neck, a specific risk of resurfacing that must be actively prevented.
The posterior surgical approach was used, with the sciatic nerve identified and protected throughout, a particular consideration given the proximity of the spinal fusion hardware and the altered anatomy it produces. At the end of the procedure, the nerve was confirmed to be tension-free.
Stability testing at the end of the operation demonstrated full range of motion, no impingement, and excellent stability, including full flexion and 90 degrees of internal rotation, confirming that the planning and execution had achieved the intended result.
The Post-Operative Result
The post-operative X-ray shows the completed bilateral hip resurfacing: the right side now matching the left, with both implants well-positioned and the joint spaces restored. The acetabular shells are well-seated, the femoral head components are capped without notching, and the overall pelvis alignment is satisfactory.
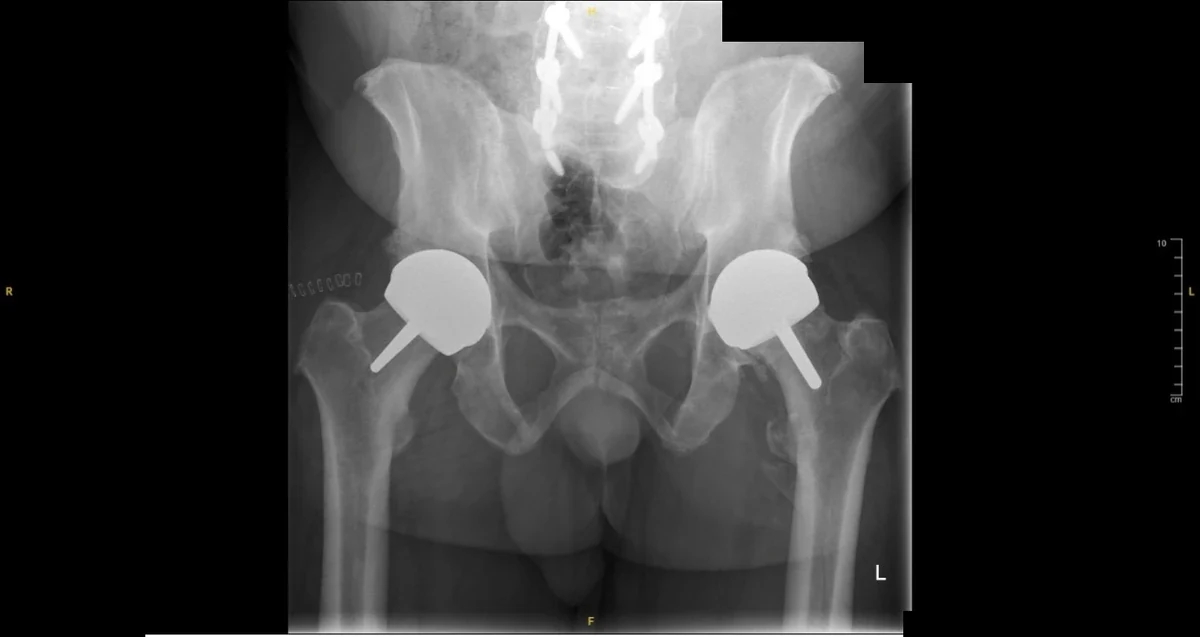
Bilateral hip resurfacing now complete. Right: newly implanted Birmingham Hip Resurfacing (54mm head, 60mm shell). Left: existing resurfacing implant. Both components well-positioned with satisfactory cup orientation. Spinal fusion metalwork unchanged.
Could This Apply to You?
This case is relevant to a growing number of patients. As spinal fusion surgery becomes more common (particularly for lumbar disc disease and spinal stenosis), more people are reaching their fifties and sixties with both a fused spine and developing hip arthritis. The two conditions frequently coexist, partly because the same underlying degenerative process affects both regions, and partly because a fused spine places increased load on the adjacent hip joints over time.
If you are in this situation, with hip pain on a background of previous spinal surgery, the important thing to know is that your options are not limited to a choice between suffering and accepting the risks of standard hip replacement. For the right patient, hip resurfacing may genuinely reduce those risks rather than add to them.
The key factors that made resurfacing the right choice in this case were:
- Good quality femoral head bone, which is essential for resurfacing to succeed
- Male sex (resurfacing outcomes are generally superior in men)
- An existing successful resurfacing on the other side, giving biomechanical symmetry
- A long spinal fusion construct with significant pelvic stiffness, making dislocation risk from standard replacement particularly high
- Metal ion levels well within safe limits, confirming the existing resurfacing was functioning correctly
- Age and activity level, both strong reasons to preserve bone stock for the long term
Not every patient with spinal fusion is a candidate for resurfacing. Older patients, those with weaker bone, and women generally have better outcomes with standard hip replacement. The decision requires careful case-by-case assessment, detailed imaging, and a surgeon with specific expertise in both resurfacing and the spinopelvic relationship.
"A complex history does not necessarily mean a compromised outcome. It means the planning must be more thorough, the surgical technique more precise, and the choice of implant more carefully considered. That is exactly where specialist expertise makes a difference."
Mr Shakir Hussain, Consultant Orthopaedic SurgeonAbout Mr Shakir Hussain
Mr Shakir Hussain is a Consultant Orthopaedic Surgeon at the Royal Orthopaedic Hospital Birmingham, specialising in hip resurfacing, complex primary hip and knee replacement, and revision surgery. He is one of a small number of surgeons in the UK performing high-volume hip resurfacing, and has specific expertise in managing patients with complex backgrounds including previous spinal surgery.
He holds the fellowship of the Royal College of Surgeons of Edinburgh in Trauma & Orthopaedics (FRCSEd Tr & Orth).
Private consultations are available at the Woodlands Suite at the Royal Orthopaedic Hospital, Priory Hospital Edgbaston, and Harborne Hospital (HCA Healthcare); all in Birmingham.